
Managing hypertension is a relentless, data-driven challenge for modern clinics. As patient populations grow and chronic conditions become more prevalent, the traditional model of relying solely on in-person visits is proving to be both clinically and financially unsustainable. The core issue lies in the gap between episodic office readings and the continuous reality of a patient’s health.
For practice managers and physicians aiming to improve patient outcomes and operational efficiency, the question is no longer if you should evolve your hypertension management program, but how. This article presents a strategic comparison between maintaining a traditional in-house model and leveraging a scalable, VMA-powered Remote Patient Monitoring (RPM) program to achieve superior clinical and financial results.
The Core Challenge: Why Traditional Hypertension Management Is Falling Short for Modern Clinics

Relying on patient visits every three to six months creates significant blind spots in care. This reactive model is inefficient and exposes both patients and practices to unnecessary risks, directly impacting your clinic’s bottom line and the well-being of your clinical team.
The Impact of Inconsistent Blood Pressure Data on Clinical Decisions
Clinical decisions made from a single, in-office blood pressure reading are like navigating with a blurry map. Was the patient nervous? Did they rush to the appointment? This “snapshot” data often fails to capture daily fluctuations, nocturnal hypertension, or the true efficacy of a medication regimen. This data gap leads to clinical inertia, delayed interventions, and an increased risk of adverse events like stroke or heart attack.
Financial Drain: The Hidden Costs of Uncontrolled Hypertension (Readmissions & No-Shows)
The consequences of poor hypertension control extend beyond clinical outcomes. Uncontrolled high blood pressure is a leading cause of preventable hospital readmissions, which can result in significant financial penalties for clinics. Furthermore, when patients feel their condition is unmanaged, it can lead to higher rates of no-shows for routine check-ups and an increase in disruptive, last-minute emergency visits, straining your administrative resources and clinical workflow.
Remote Patient Monitoring (RPM) for Hypertension: A High-Level Definition for Decision-Makers
Remote Patient Monitoring (RPM) for hypertension is a healthcare delivery model that uses technology to track patient blood pressure and other vital signs outside of the clinical setting. Patients use connected devices (like a cellular blood pressure cuff) at home, which automatically transmit real-time data to healthcare providers. This allows for continuous oversight, early detection of potential issues, and proactive care management, transforming hypertension care from a reactive to a proactive process.
In-House Care vs Remote Monitoring: A Comparative Analysis for Clinic Operations
Choosing the right model for scaling your hypertension program requires a clear-eyed look at data, cost, and patient engagement. While in-house staff are invaluable, their traditional role in chronic care management has operational limits that a VMA-powered RPM model is designed to overcome.
Data Frequency & Accuracy: Episodic Visits vs Real-Time Daily Monitoring
- In-House Model: Relies on data collected sporadically during office visits. This data is prone to “white coat syndrome” and provides no insight into a patient’s daily life, creating significant gaps in understanding.
- RPM Model: Captures a steady stream of daily readings from the patient’s home environment. This provides a far more accurate and comprehensive view of their condition, allowing for precise medication titration and timely lifestyle interventions.
Cost Structure: High Overhead of In-Person Staff vs Scalable Virtual Support
- In-House Model: Requires dedicated clinical staff (RNs, MAs) to manage patient check-ins, follow-up calls, and data entry. This involves high, fixed overhead costs including salaries, benefits, and office space, which do not easily scale.
- RPM Model: Leverages a flexible, scalable workforce of Virtual Medical Assistants. This shifts the cost from a fixed overhead to a variable operational expense, allowing your clinic to manage a larger patient panel without a proportional increase in headcount. To understand the financial and operational differences, it’s helpful to compare a Virtual Medical Assistant vs. In-House Staff directly.
Patient Engagement: The Limits of In-Person Motivation vs Consistent Digital Touchpoints
- In-House Model: Patient motivation and education are confined to brief interactions during appointments. Between visits, adherence can wane without consistent reinforcement.
- RPM Model: Creates daily opportunities for engagement. Automated reminders, educational content, and follow-ups from a Virtual Medical Assistant keep patients actively involved in their own care, improving adherence and outcomes.
The Implementation Hurdle: Why RPM Fails Without the Right Operational Support
Many clinics are intrigued by the promise of RPM but hesitate due to perceived operational burdens. They are right to be cautious. Simply deploying devices without a robust workflow to manage the resulting data is a recipe for failure.
The Myth of “Set It and Forget It”: Managing Data Overload and False Alerts
A successful RPM program generates a massive amount of data. Without a system to filter and prioritize this information, your clinical team can quickly become overwhelmed by data noise and alert fatigue, causing them to ignore critical signals.
The Staffing Gap: Who Is Responsible for Daily Patient Monitoring and Triage?
This is the most critical question for any clinic considering RPM. Is your already busy nursing staff expected to monitor incoming data streams all day? Who will triage the alerts, contact patients for context, and decide what needs to be escalated to a physician? Piling these tasks onto your existing team leads to burnout and defeats the purpose of improving efficiency.
The Solution: Integrating Virtual Medical Assistants into Your Hypertension RPM Workflow
This is where the model shifts from simply “using RPM” to strategically scaling care with VMA support. A trained, HIPAA-compliant Virtual Medical Assistant from Care VMA acts as the operational engine for your RPM program, handling the daily monitoring and triage so your clinical team can focus on top-of-license tasks. You can explore The Ultimate Guide to Healthcare Virtual Assistants to see the wide range of tasks they can manage.
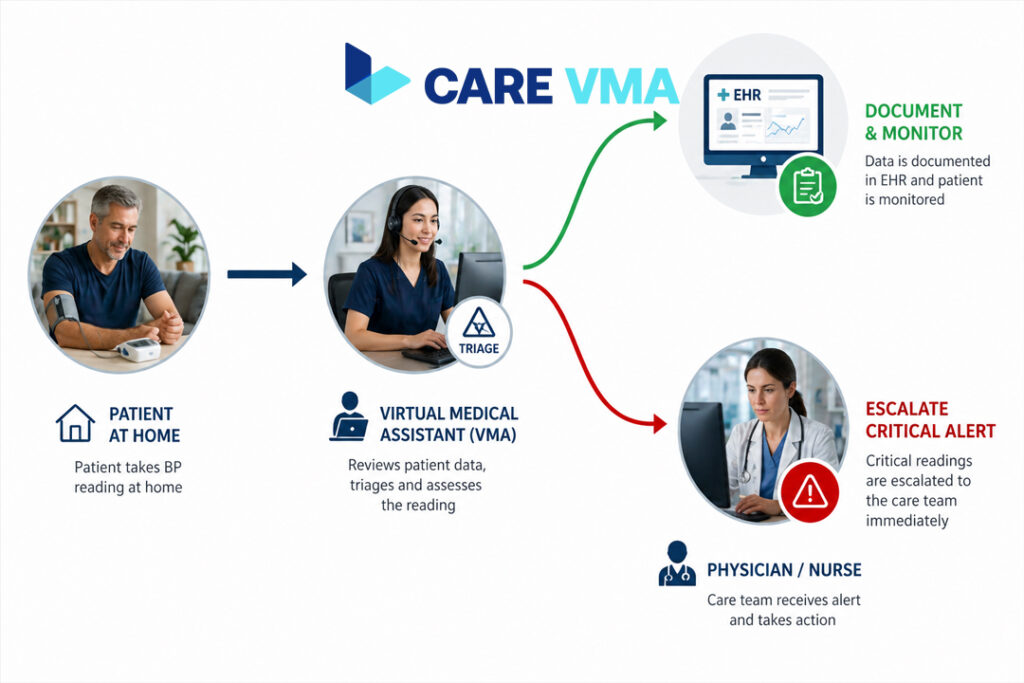
Use Case: The VMA-Powered RPM Workflow for a Hypertensive Patient
Consider a typical workflow for a patient enrolled in your program, streamlined to ensure efficiency and safety. This structured approach is key to a successful RPM workflow for clinics.
- Before VMA: Reactive care based on sporadic in-office readings, high staff burden. Your front desk and medical assistants are bogged down with manual follow-up calls and scheduling, while nurses spend valuable time chasing down routine data instead of managing complex cases.
- After VMA: Proactive intervention based on daily data trends, streamlined alerts for clinical staff, and improved patient adherence. A Care VMA monitors the incoming BP readings daily. They document normal readings in the EHR, contact the patient for clarification on slightly elevated readings (e.g., “Did you just exercise?”), and only escalate clinically significant alerts to your in-house nurse according to pre-defined protocols.
Calculating the ROI of a VMA-Powered RPM Program for Hypertension
A VMA-powered RPM program isn’t a cost center; it’s a revenue and efficiency driver. The return on investment is measured through reduced costs, improved reimbursements, and optimized staff allocation.
Quantifying the Reduction in Hospital Readmission Penalties
By proactively identifying and managing BP spikes, your clinic can significantly reduce hypertension-related emergency room visits and hospitalizations. This directly protects your practice from costly readmission penalties and improves your quality metrics.
Modeling the Financial Impact of Improved Staff Efficiency and Focus
Calculate the hourly cost of your registered nurses and medical assistants. How many of their current hours are spent on routine, administrative tasks related to hypertension follow-up? By offloading daily monitoring, patient reminders, and initial triage to a cost-effective VMA, you free up your expensive clinical resources to perform reimbursable procedures, manage more complex patients, and operate at the top of their license.
Optimizing Your Clinic’s Scheduling and Reducing Missed Appointments
A well-managed RPM program has a powerful secondary benefit: a more predictable and efficient clinic schedule.
How Consistent Monitoring Reduces Unnecessary Emergency Visits
When patients feel connected and monitored, they are less likely to make a panicked trip to the emergency room for a high reading they took at a pharmacy. Instead, they trust the system, knowing that a VMA is monitoring their data and will facilitate a clinical response if needed.
Using VMA-led follow-ups to ensure adherence to scheduled appointments post-alert.
When a VMA escalates a series of concerning readings to your nurse, a follow-up appointment is often necessary. The VMA can handle the entire scheduling process, ensuring the patient is booked promptly. They can also perform reminder calls, reducing the no-show rate for these critical visits and ensuring the care loop is closed.
Ensuring Trust and Security: HIPAA Compliance in VMA-Assisted Patient Monitoring
Patient data security is non-negotiable. Partnering with a professional organization ensures that every aspect of your RPM program is built on a foundation of trust and compliance.
Data Security Protocols for Transmitting Blood Pressure Readings
Care VMA utilizes secure, encrypted platforms for all data transmission. Our processes are designed to meet or exceed all technical safeguards required by HIPAA, ensuring that your patients’ protected health information (PHI) is secure at every stage.
Training and Professional Standards for Care VMA’s Virtual Assistants
Our Virtual Medical Assistants are not administrative generalists; they are healthcare professionals trained in medical terminology, privacy protocols, and the specific workflows of a clinical environment. You can be confident you are working with HIPAA Compliant Virtual Assistants who understand the gravity of their role in patient care.
Partner with Care VMA: Build a Scalable and Profitable Hypertension Management Program
Stop stretching your in-house team thin and start building a more resilient, proactive, and profitable chronic care program. By integrating Care VMA’s trained virtual assistants into your RPM workflow, you can scale your capacity, improve patient outcomes, and reduce staff burnout.
- Step 1: Schedule a No-Obligation Consultation to Analyze Your Current Workflow Let’s discuss your current challenges, patient panel size, and strategic goals.
- Step 2: Receive a Custom Implementation Blueprint for Your Clinic We’ll design a VMA-powered RPM workflow tailored to your specific needs, EMR system, and clinical protocols.
- Step 3: Launch Your VMA-Powered RPM Program in as Little as Two Weeks Our streamlined onboarding process ensures a smooth transition, allowing you to quickly start realizing the benefits of a more efficient and effective hypertension management system.
Schedule Your Free Consultation Today
Frequently Asked Questions (FAQ)
How do Virtual Medical Assistants triage incoming blood pressure alerts?
VMAs operate under protocols established by your clinic. They are trained to differentiate between non-urgent readings needing documentation, readings requiring patient clarification (e.g., checking for user error or context), and clinically significant alerts that must be immediately escalated to your on-site clinical staff.
What is the typical cost difference between hiring an in-house nurse for monitoring versus using a VMA service?
Using a VMA service is significantly more cost-effective. You avoid the high overhead costs of a full-time employee, such as salary, benefits, payroll taxes, and paid time off. With a VMA, you pay only for the productive time required to manage your patient panel, providing a scalable solution that aligns costs directly with your program’s size.
How does your VMA service integrate with our existing EHR system for hypertension data?
Our VMAs are trained on a wide variety of major EHR systems. They can securely access your system to document patient readings, update notes, and manage scheduling, ensuring seamless data flow and maintaining a single source of truth for patient records.
Can a VMA handle patient education and follow-up for medication and lifestyle adherence?
Yes. While VMAs do not provide medical advice, they can execute communication plans developed by your clinical team. This includes making follow-up calls to remind patients about medication schedules, providing approved educational materials, and documenting patient-reported adherence, all of which saves your clinical staff valuable time.
What is the process for onboarding patients onto the RPM platform with a VMA’s assistance?
Our VMAs can manage the administrative aspects of patient onboarding. This includes outreach to eligible patients, explaining the benefits of the program, walking them through the enrollment process, and coordinating the shipment and setup of their RPM devices, ensuring a smooth and positive start for your patients.
