
The promise of Remote Patient Monitoring (RPM) is immense: better outcomes for chronic care patients, new revenue streams, and a proactive approach to healthcare. But for many clinic managers and physicians, the reality is a logistical nightmare. The threat of overwhelming your already-burnt-out staff with data review, tech support, and complex billing rules makes the entire program feel unsustainable.
An RPM workflow is a structured, five-phase clinical process that enables clinics to monitor patient vitals remotely, intervene proactively, and ensure compliant billing. An efficient workflow automates administrative tasks to reduce staff burden, using clear protocols for patient identification, onboarding, daily monitoring, clinical intervention, and billing reconciliation to create a sustainable and profitable program.
Stop theorizing about RPM—this is the actionable 5-phase clinical workflow that prevents staff burnout and ensures you get paid. We’ll detail each step and show you how a HIPAA-compliant Virtual Medical Assistant can automate the administrative burden, transforming your RPM program from a source of stress into a seamless, profitable extension of your practice.
The 5 Clinical Phases of an Efficient RPM Workflow
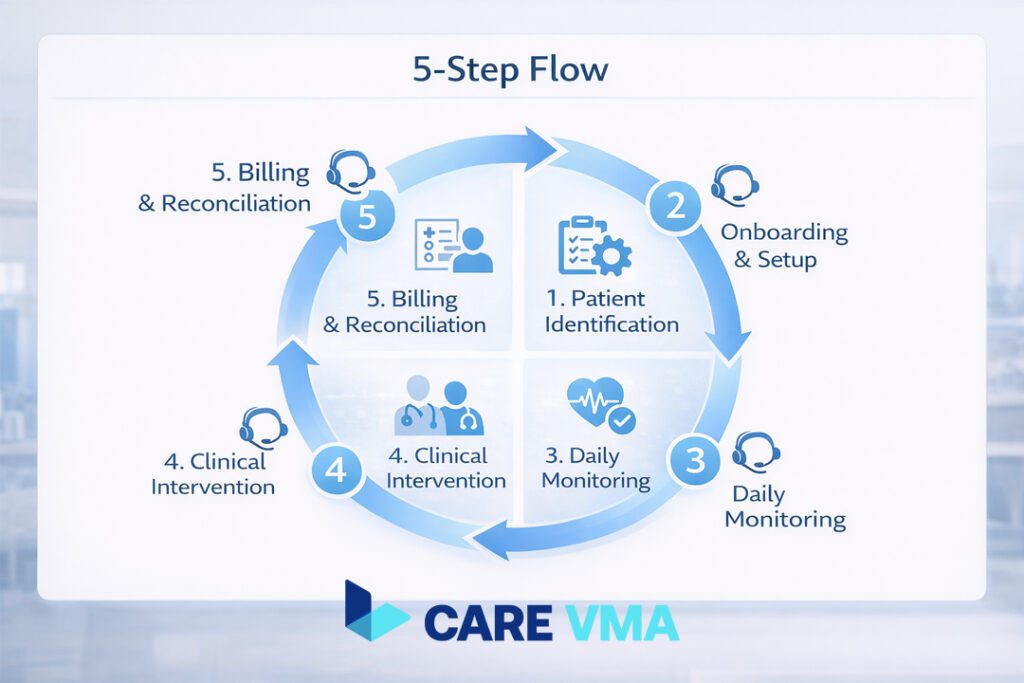
A successful remote patient monitoring program isn’t just about the technology; it’s about the operational system you build around it. By breaking the process into five distinct clinical phases, you can assign clear responsibilities, eliminate ambiguity, and create a repeatable, scalable model.
Phase 1: Patient Identification & Enrollment
Goal: To build a high-adherence patient panel without manual chart-digging.
This is where most practices struggle first. Manually sifting through hundreds of patient charts to find eligible candidates is a non-starter for a busy clinic. The key is to systematize identification and make enrollment a natural part of the clinical conversation.
In-Practice Execution:
- Eligibility Filtering (The VMA’s Role): A trained VMA runs a pre-built, customized query in your EHR. This query filters for patients who meet specific criteria, such as having two or more chronic conditions (e.g., Hypertension, CHF, Diabetes) and being covered by Medicare or a specific commercial plan.
- Clinical Review (The Clinician’s Role): The VMA presents this filtered, high-potential list to the lead RN or physician. The clinician performs a quick review, using their judgment to approve candidates who are most likely to benefit and adhere to the program.
- The Warm Handoff (The Physician’s Role): During the patient’s next scheduled visit, their trusted physician introduces the RPM program. This is not a sales pitch; it’s a clinical recommendation framed around benefits like “better control over your blood pressure between visits” or “helping us catch issues before they become serious.”
- Consent & Enrollment (The MA or VMA’s Role): Once the patient agrees, an in-office Medical Assistant can obtain the necessary verbal or written consent and finalize the enrollment paperwork. For telehealth-based practices, a VMA can manage this process using secure digital consent forms and follow-up calls.
Pro-Tip: Patient enrollment rates increase by over 50% when the recommendation comes directly from their physician during an established visit, leveraging the existing patient-provider trust.
Phase 2: Patient Onboarding & Device Setup (CPT 99453)
Goal: A frictionless, tech-support-free setup that empowers the patient and ensures data transmission from day one.
The single biggest point of failure in many RPM programs is patient-facing technology. Complicated Bluetooth pairing, Wi-Fi connectivity issues, and app troubleshooting can quickly consume your staff’s time. The workflow must be designed to eliminate these hurdles.
In-Practice Execution:
- Device Logistics (The VMA’s Role): Your VMA coordinates directly with your chosen device partner to ship a pre-configured cellular device kit to the patient’s home. These “plug-and-play” devices work out of the box—no pairing, Wi-Fi, or smartphone app is needed. This simple step reduces patient tech support calls by over 70%.
- Patient Education: In the clinic, an MA demonstrates how to use the device (e.g., a blood pressure cuff) and take a proper reading. They crucially explain that RPM is for routine monitoring, not an emergency service. For remote setups, this can be done via a telehealth call or a simple instructional video.
- First Reading Confirmation: The MA or a telehealth virtual assistant has the patient take their first reading before they leave the office (or during the welcome call) to confirm that data is transmitting successfully to the RPM platform.
Compliance Alert: CPT 99453 (Initial Setup & Education) is a one-time billable code. To be compliant, you must document that the patient has been educated and has successfully transmitted at least one reading.
Phase 3: Daily Monitoring & Triage (CPT 99454)
Goal: To catch clinical risks early without creating data-fatigue for your nurses.
Your clinical staff cannot be expected to watch a dashboard all day. An effective monitoring workflow separates the “noise” from the “signal,” allowing nurses to focus only on the data that requires their clinical expertise.
In-Practice Execution:
- Automated Data Review (The VMA’s Role): The VMA is the first line of defense. They monitor the RPM dashboard daily. Over 90% of incoming readings are typically “Green” (within normal, pre-set parameters). The VMA reviews, documents these as “reviewed,” and moves on. No clinical time is spent on normal data.
- Alert Triage Protocol:
- Yellow Alerts (e.g., missed readings, minor deviations): The VMA initiates a standardized protocol. For a missed reading, they might send a pre-approved SMS reminder. If there’s no reading after 24 hours, the VMA flags the patient for a check-in call from the RPM nurse.
- Red Alerts (e.g., a critically high blood pressure reading): The platform should automatically send an immediate notification (via EHR inbox, secure message, or SMS) directly to the on-call RPM Nurse for immediate clinical action.
- The 16-Day Rule (The VMA’s Role): To bill CPT 99454, CMS requires data transmission on at least 16 days of a 30-day period. The VMA actively tracks this for each patient. If a patient is at risk of missing this threshold, the VMA proactively flags them for an engagement call from the team, protecting your revenue.
This division of labor is a core strategy for preventing physician burnout and keeping your RPM program sustainable.
Phase 4: Clinical Intervention & Management (CPT 99457/99458)
Goal: To deliver timely, billable care based on RPM data and document it perfectly.
This is where clinical value is created and revenue is captured. When a nurse or physician spends time acting on RPM data, that time is often billable. The workflow must make it easy to perform the intervention and effortless to track the time.
In-Practice Execution:
- Automated Time-Tracking (The VMA’s Role): Modern RPM platforms can automatically start a timer the moment a clinician opens a patient’s file to review an alert or initiates a call. A VMA ensures this time is logged correctly, with associated notes, making the entire process audit-proof for billing CPT 99457 (the first 20 minutes) and 99458 (each additional 20 minutes).
- Intervention (The Nurse’s Role): The RPM nurse receives the “Red Alert” escalation. They contact the patient to assess symptoms, review medication adherence, and provide clinical guidance according to the practice’s established standing orders.
- Documentation and Escalation: The nurse documents the interaction, findings, and time spent in the platform. If the situation requires a medication change or a higher level of care, they escalate the case to the physician or NP. This interaction seamlessly becomes part of the EHR/EMR management record.
Staff burnout is the #1 reason RPM programs fail. See how a Care VMA handles 90% of the daily monitoring tasks, freeing your nurses for critical patient care that only they can provide.
Phase 5: Billing & Reconciliation
Goal: To guarantee 100% compliant reimbursement with minimal manual effort from your billing staff.
At the end of the month, your billing team shouldn’t have to hunt through spreadsheets or manual time logs. The workflow should deliver a clean, simple, and defensible billing report.
In-Practice Execution:
- The End-of-Month Audit (The VMA’s Role): On the last business day of the month, the VMA generates an automated billing report from the RPM platform. This report validates two key data points for each patient:
- Did they transmit data on ≥16 days? (Required for CPT 99454)
- Did they receive ≥20 minutes of interactive care time? (Required for CPT 99457)
- Clean Claim Generation: The report gives your biller a simple, “ready-to-bill” list of patients and the exact CPT codes to be charged. A medical billing virtual assistant can then prepare and submit these claims, cross-referencing the automated report which contains all necessary supporting documentation (time logs, communication notes).
For reference, here are the primary RPM codes and their average 2026 Medicare reimbursements.
| CPT Code | Description | Key Requirement | Avg. Reimbursement |
|---|---|---|---|
| 99453 | Initial Setup & Education | One-time, per episode of care | ~$20 |
| 99454 | Device & Data Supply | At least 16 days of data/month | ~$50/month |
| 99457 | First 20 Min. of Care | 20 mins of interactive time/month | ~$50/month |
| 99458 | Add’l 20 Min. of Care | Each additional 20 mins/month | ~$40/increment |
Putting It All Together: Your VMA-Powered RPM Team
An efficient RPM workflow isn’t about adding more work; it’s about reallocating work to the right resources. By integrating a VMA, you create a system where everyone operates at the top of their license.
- Physicians/NPs make clinical decisions and provide oversight.
- RPM Nurses manage high-risk patients and perform clinical interventions.
- MAs handle in-person patient interactions and education.
- Virtual Medical Assistants manage patient identification, device logistics, non-clinical data review, compliance tracking, and billing preparation.
This model makes your RPM program operationally light, financially sound, and clinically effective. It reduces administrative workload, ensures near-perfect billing compliance, and improves patient adherence—making your program sustainable and scalable for the long term.
Ready to Build an Effortless RPM Workflow?
Stop letting administrative complexity hold you back. An RPM program should support your clinic, not burden it. When powered by a smart, automated workflow and the right support team, it can become a powerful tool for improving patient outcomes and practice health.
Schedule a free, no-obligation workflow consultation with our specialists. We’ll help you map out these 5 phases for your specific practice and show you how a VMA can make it effortless.
