
Are claim denials, delayed payments, and administrative overload impacting your clinic’s cash flow? The root of the problem might not be your billing team, but a process that happens long before an invoice is ever sent: medical coding. In a busy practice, it’s a detail that’s easy to overlook, yet it dictates whether you get paid fully, partially, or not at all.
Medical coding is the process of translating clinical documentation—physician’s notes, diagnoses, procedures, and medical services—into universal alphanumeric codes. Think of it as the financial language of healthcare. This translation is the single most critical step in the revenue cycle, turning your team’s clinical work into accurate reimbursement. Without the right translation, your clinic’s financial health is at risk.
Key Takeaways for Clinic Operations:
- Purpose: To create a standardized claim that tells payers precisely what services were performed and why they were medically necessary.
- Process: Coders analyze clinical notes and assign specific codes from sets like ICD-10, CPT, and HCPCS Level II.
- Impact: Medical coding directly affects your clinic’s cash flow, operational efficiency, and compliance with healthcare regulations.
Beyond Definitions: Why Medical Coding is the Engine of Your Revenue Cycle
Think of every patient encounter as a story. The physician documents the patient’s history, symptoms, examination, diagnosis, and the treatment provided. Medical coding is how you translate that clinical story into a structured language that payers—like insurance companies, Medicare, and Medicaid—understand and use to process payments.
This is where many practices struggle. An incorrect or non-specific code can break the entire chain, leading to a cascade of administrative problems.
- Connecting Clinical Work to Financial Reimbursement: Accurate codes justify medical necessity, proving to the payer that a service was warranted. A clean claim, supported by precise codes, gets processed and paid quickly.
- The High Cost of Inaccuracy: A coding error almost always results in a claim denial. This doesn’t just delay payment; it creates a mountain of administrative rework. Your staff must then investigate the denial, query the physician, correct the code, and resubmit the claim—a time-consuming process that cripples both productivity and cash flow. This is a core component of effective denial management and prevention.
- Data for Better Operations: Beyond billing, coding data provides valuable insights into your practice. It helps you track which services are most common, analyze patient population health trends, and make informed decisions about resource allocation.
The Anatomy of a Claim: The 3 Core Code Sets Every Clinic Manager Should Know
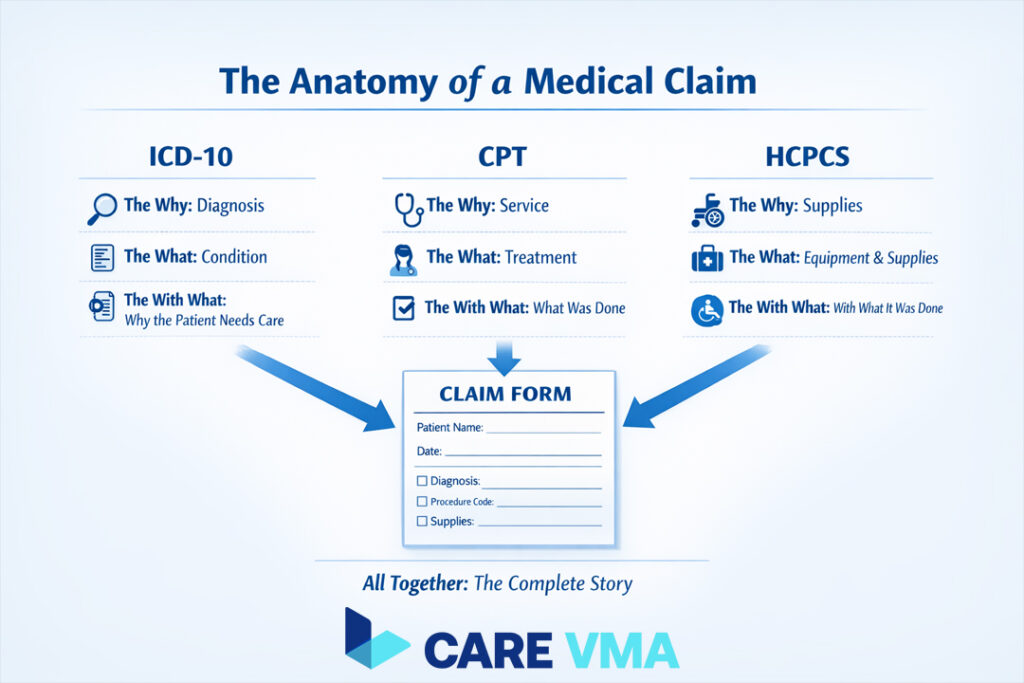
To an administrator, the alphabet soup of medical codes can seem overwhelming. However, understanding their distinct roles is crucial for overseeing your revenue cycle. There are three main code sets that work together on every claim.
The “Why”: ICD-10-CM Codes for Diagnoses
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) codes answer the question, “Why did the patient need care?” They represent diagnoses, symptoms, and conditions. These codes establish the medical necessity for any services provided.
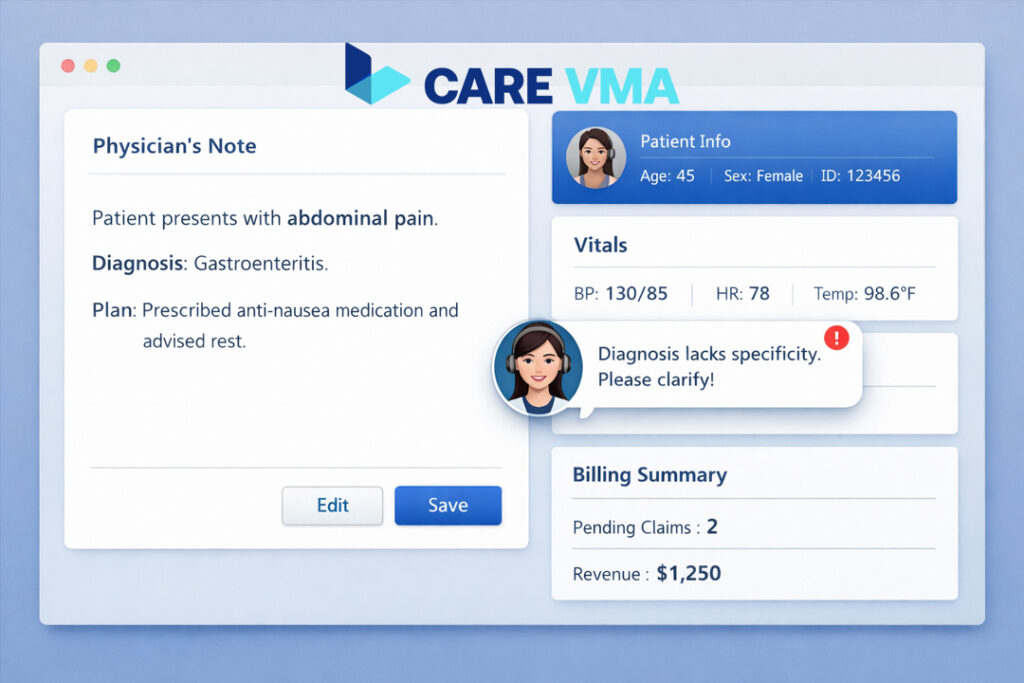
Operational Insight: Specificity is non-negotiable. Submitting a claim with a vague code like R51.9 (Headache, unspecified) for an established patient is a recipe for denial. A more specific code, like G43.909 (Migraine, unspecified, not intractable, without status migrainosus), provides the detail payers require and significantly increases the chances of first-pass payment.
The “What”: CPT Codes for Procedures & Services
CPT (Current Procedural Terminology) codes answer the question, “What did the provider do?” Maintained by the American Medical Association (AMA), these five-digit numeric codes describe every service performed, from an office visit to a complex surgical procedure.
Examples include:
- 99213: A standard office visit for an established patient.
- 71045: A single-view chest X-ray.
- 12001: Simple repair of a superficial wound (2.5 cm or less).
The “With What”: HCPCS Level II Codes for Supplies & Equipment
HCPCS (Healthcare Common Procedure Coding System) Level II codes answer, “What supplies, drugs, or equipment were used?” These alphanumeric codes cover items not included in CPT, such as:
- Durable medical equipment (DME) like crutches or wheelchairs.
- Ambulance services.
- Prosthetics and orthotics.
- Specific drugs administered in the office.
A Day in the Life: The Medical Coding Workflow in a Modern Clinic
Understanding the workflow is the key to identifying and fixing bottlenecks in your revenue cycle. It’s not a single event but a multi-step process that relies on seamless communication between your clinical and administrative teams.
Here’s a breakdown of the journey from a clinical note to a payable claim:
- Step 1: The Patient Encounter & Physician Documentation The process begins in the exam room. The physician sees the patient and documents the encounter in the Electronic Health Record (EHR), detailing the history, exam, medical decision-making, diagnosis, and any procedures performed.
- Step 2: The Hand-off to the Coder Once the physician signs off on the note, the patient chart enters the coding queue. This is the critical transfer of information. The quality of the documentation at this stage dictates the success of every subsequent step.
- Step 3: Abstracting the Record & Assigning Codes A remote medical coder or in-house specialist reviews the entire chart. They “abstract” the key information—the primary diagnosis, secondary conditions, services rendered—and translate it into the appropriate ICD-10, CPT, and HCPCS codes.
- Step 4: The Coder-Physician Query Loop (A Common Bottleneck) It sounds simple, but this is where delays often begin. If a physician’s note is vague, lacks specificity, or is contradictory, the coder cannot assign an accurate code. They must then send a query back to the provider for clarification.
Workflow Watchpoint: The query loop is a major source of operational drag. A busy physician may take hours or even days to respond, halting the entire billing process. This delay directly increases the time a claim sits in Accounts Receivable (A/R).
- Step 5: Finalizing Codes for Claim Submission Once all information is clarified and the codes are confirmed, they are entered into the practice management system. The medical billing team then uses these codes to generate and submit the final claim to the payer.
Medical Coding vs Medical Billing: Two Sides of the Same Coin
Many clinic managers use the terms “coding” and “billing” interchangeably, but they are fundamentally different roles. Understanding the distinction is crucial for effective revenue cycle management (RCM).
A coding mistake creates an impossible task for the biller. If the coder provides the wrong “translation,” the biller will inevitably submit a flawed claim that gets denied, forcing the entire process to start over.
| Function | Medical Coder (The Translator) | Medical Biller (The Financial Officer) |
|---|---|---|
| Primary Role | Analyzes clinical documentation to assign standardized codes. | Creates and submits claims to payers using the assigned codes. |
| Focus | Accuracy of the clinical story. | Accuracy of the financial claim and collection. |
| Output | A set of validated ICD-10 and CPT codes. | A submitted claim, patient statements, and payment follow-up. |
For a deeper dive into how these two critical functions differ and interact, explore our guide on Medical Billing vs. Medical Coding.
How Flawed Coding Silently Drains Your Clinic’s Resources
These three common coding mistakes might be costing your practice thousands each month, not just in lost revenue but in wasted administrative time.
- Lack of Specificity: This is the most frequent cause of denials. Payers require the highest possible level of detail. Coding for “diabetes” (E11.9) when the chart specifies “Type 2 diabetes with diabetic neuropathy” (E11.40) will trigger an immediate rejection for more information.
- Unbundling Services: This occurs when procedures that should be billed under a single, comprehensive code are billed separately. While it may seem like a way to increase reimbursement, payers view it as a fraudulent practice that can trigger costly audits.
- Incorrect Use of Modifiers: Modifiers are two-digit codes added to a CPT code to provide additional information about a service (e.g., indicating a procedure was performed on the left side of the body). Using the wrong modifier or forgetting one altogether causes payment delays and requires manual rework.
Automating Accuracy: The Role of Virtual Medical Assistants in Your Coding Workflow
How can a busy practice solve the bottlenecks of documentation queries and pre-submission errors without hiring more staff? This is where technology and specialized remote support become a game-changer. A Virtual Medical Assistant (VMA) integrates into your workflow to provide proactive support.
- Bridging the Documentation Gap: Instead of a coder chasing down a physician days later, a VMA can be tasked with reviewing charts for completeness before they even enter the coding queue. They can flag notes that lack specificity and prompt the provider for clarification while the patient encounter is still fresh in their mind.
- Pre-submission Audits: A VMA trained in RCM can perform a preliminary review of codes against payer-specific rules, catching potential errors related to modifiers or bundled services before the claim is ever submitted. This dramatically increases your “clean claim rate.”
- Reducing Administrative Load: By handling these administrative checks, a VMA frees your certified coders to focus on complex, high-value cases. Your billers, in turn, spend less time chasing denials and more time managing payments.
Building a Compliant and Efficient Coding Process
For clinic managers and physician-owners, mastering medical coding isn’t about becoming a certified coder yourself. It’s about understanding the system so you can build a workflow that protects your revenue and frees your team from administrative headaches.
Actionable Takeaways for Clinic Leadership:
- Invest in Certified Talent: Whether in-house or remote, ensure your coding is handled by AAPC or AHIMA certified professionals who are up-to-date on the latest regulations.
- Foster Coder-Physician Communication: Create a streamlined, respectful query process. Emphasize that a coder’s request for detail is an effort to ensure the physician is fully reimbursed for their work.
- Leverage Technology: Integrate solutions like what a virtual medical assistant can do to handle the administrative pre-checks and communication that slow down your revenue cycle.
If you’re ready to build a more efficient and profitable revenue cycle, a managed solution can make all the difference. A Virtual Medical Assistant from Care VMA Health can take on the administrative burden of your coding and billing process, helping you reduce claim denials and accelerate cash flow.
Schedule a free, no-obligation consultation today to discover how we can optimize your clinic’s operations.
