
Every year, the complex web of CPT codes and CMS reimbursement rules shifts, threatening your practice’s revenue with hidden cuts and a higher risk of claim denials. The 2026 updates, however, are particularly significant, introducing a -2.5% “efficiency adjustment,” a complete overhaul of critical vascular codes, and confusing dual conversion factors. Ignoring these details isn’t an option—it’s a direct path to revenue loss. This guide is designed to cut through that complexity, providing you with clear, actionable strategies to protect your practice and secure every dollar you’ve rightfully earned.
The CPT Coding & Reimbursement Rules for 2026 introduce significant changes from the AMA and CMS, including 418 total code updates, a -2.5% “efficiency adjustment” cut to the work RVUs for most non-time-based services, and 46 new codes for lower extremity revascularization (LER). A deep understanding of how these new coding and payment rules interact is essential for maximizing payments and ensuring full compliance in the year ahead. This guide, based on an expert analysis of the official AMA CPT® 2026 Code Set and the 2026 Medicare Physician Fee Schedule (MPFS) Final Rule, has been reviewed by our team of certified medical coders to provide you with the most reliable and practical insights.
Understanding the Basics: How CPT & RVU Determine Your Revenue
At first glance, the formula for how you get paid might seem overwhelmingly complex. But in reality, it boils down to a few key components that every practice manager and provider must understand to navigate the financial landscape of healthcare. Getting this right is the foundation for surviving the 2026 changes.
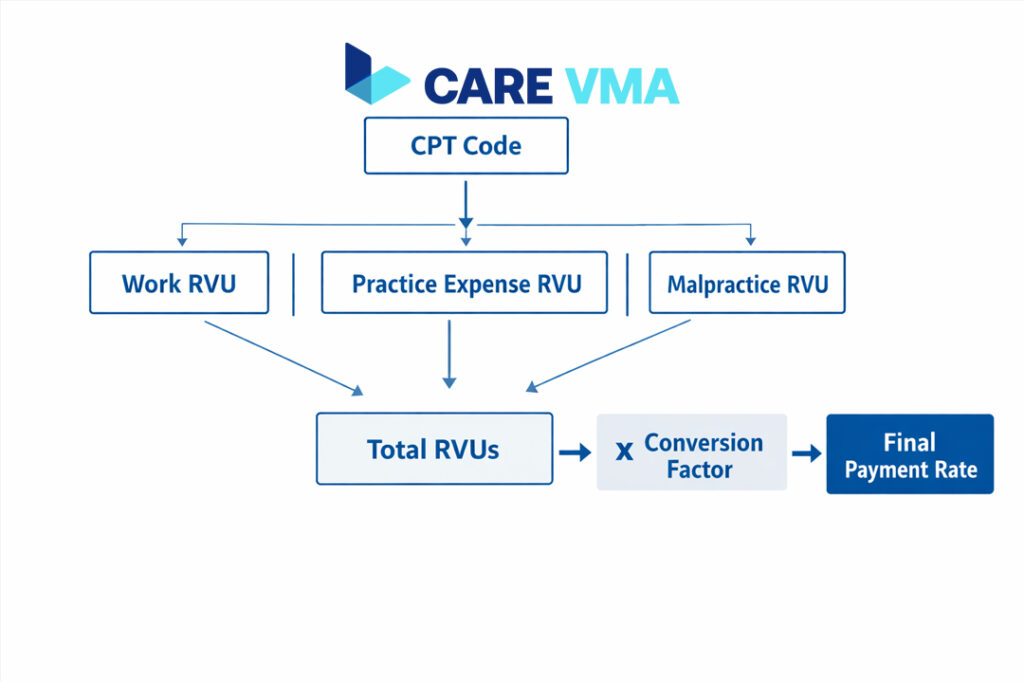
The entire system hinges on the relationship between the service you provide, the code you assign, and the value Medicare places on it. The American Medical Association (AMA) creates and maintains the Current Procedural Terminology (CPT) codes—the universal language for medical services. Each of these codes is then assigned a value by the Centers for Medicare & Medicaid Services (CMS), calculated using Relative Value Units (RVUs).
RVUs are composed of three parts:
- Physician Work (wRVU): The time, skill, and intensity required to perform the service.
- Practice Expense (peRVU): The costs of running the practice, such as rent, equipment, supplies, and staff salaries.
- Malpractice (mpRVU): The cost of professional liability insurance.
Once the total RVUs are calculated, they are multiplied by a national Conversion Factor (CF)—a dollar amount that changes annually—to determine the final payment rate.
The Biggest CPT 2026 Changes: What Most Impacts Your Practice?
Not all of the 418 code updates are created equal. Here’s the thing: while some are minor revisions, a few key areas have been completely overhauled. These are the changes for 2026 that carry the highest operational risk—and the greatest opportunity—for your bottom line if managed correctly.
Perombakan Total Kode Revaskularisasi Ekstremitas Bawah (LER)
Perhaps the most significant surgical coding change for 2026 is the complete deletion of the familiar Lower Extremity Revascularization (LER) codes (37220-37235). They have been replaced with a complex set of 46 new territory-based codes (37254-37299).
This isn’t just a simple code swap. The new system is far more granular, requiring precise documentation of:
- Vascular Territory: Interventions are now defined by one of four territories: iliac, femoral/popliteal, tibial/peroneal, and inframalleolar.
- Lesion Complexity: Coders must now distinguish between a “straightforward” lesion (stenosis) and a “complex” lesion (occlusion).
This change makes accurate and detailed physician documentation more critical than ever. An incorrect or incomplete report can easily lead to downcoding or an outright denial, making this a top area of concern for denial management in 2026.
The New Era of Digital Health & Remote Monitoring
The 2026 CPT updates solidify the role of digital health in mainstream care. Acknowledging that patient monitoring isn’t always a month-long process, new codes like 99445 have been introduced to report short-duration Remote Patient Monitoring (from 2 to 15 days).
Furthermore, the time threshold for management services has been lowered. For instance, code 99470 now supports remote monitoring treatment management after just 10 minutes of service per month, down from the previous 20-minute requirement. This reflects a move toward valuing shorter, more efficient digital interactions. For more information, our guide on the benefits of remote patient monitoring offers a deeper dive.
The Arrival of AI Category I Codes
For the first time, artificial intelligence-augmented services have been elevated to Category I status, signaling that payers now recognize them as a standard of care. New codes have been established for AI-augmented diagnostics, including software that performs:
- Coronary atherosclerotic plaque analysis.
- Cardiac risk assessment from perivascular fat.
- Classification of burn wounds from multispectral imaging.
To justify these new codes, documentation must clearly specify that an AI-driven analysis was used to support the physician’s work, a new requirement that your clinical and coding teams must be prepared for.
CMS 2026 Reimbursement Rules: The Cuts and Changes That Will Reshape Your Revenue
What most providers don’t realize is that code changes are only half the battle. The real financial impact often comes directly from the CMS Medicare Physician Fee Schedule (MPFS) Final Rule, which dictates how those codes are actually paid. The 2026 rule introduces some game-changing financial policies.
Waspada: The Hidden “-2.5% Efficiency Adjustment”
The most alarming change for many practices is the finalization of a -2.5% “efficiency adjustment” applied to the work RVUs of nearly all non-time-based services.
Here’s what that means in practice:
- Impacted Services: The cut directly affects payment for most surgical procedures, diagnostic tests, and radiology services.
- Exempted Services: Crucially, time-based services like Evaluation and Management (E/M) visits and many behavioral health services are exempt from this specific cut for 2026.
This policy creates a clear financial incentive to ensure that all time-based encounters are documented and coded with absolute precision to help offset the revenue lost from procedural services.
Dual Conversion Factors: Who Gets Paid More?
In another major shift, CMS is implementing two separate Conversion Factors (CF) for 2026, creating a tiered payment system. The rate you receive will depend on your participation in an Alternative Payment Model (APM).
- Qualifying APM Participants (QPs): Receive a higher CF of approximately $33.57.
- Non-QP Clinicians: Receive the standard CF of approximately $33.40.
While both rates represent a slight increase from 2025, this dual structure is a clear signal from CMS encouraging providers to move toward value-based care models.

Other Changes to Note: Telehealth & Virtual Supervision
On a more positive note, CMS has finalized several pandemic-era telehealth policies. The policy allowing “direct supervision” to be met via real-time audio/video technology has been made permanent. Additionally, the popular E/M complexity add-on code, G2211, has been expanded for use with home and residence visits, supporting longitudinal care for homebound patients.
From Theory to Practice: Care VMA’s Strategies to Protect Your 2026 Revenue 🔥
Knowing the rules is one thing; protecting your revenue from these complex changes is another. This is where a strategic approach becomes indispensable. In many cases, practices try to manage this burden internally, but that reactive model often leads to burnout and lost revenue. Here’s how a dedicated partner turns this compliance headache into a financial advantage.
Automating Code Updates & Avoiding LER Denials
With 46 new and highly specific LER codes, the risk of manual error is immense. The Care VMA platform, managed by our team of certified vascular coders, proactively updates your chargemaster and internal systems. We build in automated coding edits that flag common mistakes with stenosis vs. occlusion documentation or incorrect territory assignment before the claim is ever submitted, drastically reducing your denial rate for these high-value procedures. This is a core part of how we approach denial management and prevention.
Fighting the -2.5% Cut with Time-Based Code Optimization
The -2.5% cut on procedural codes makes accurate time-based coding more important than ever for your practice’s financial health. A virtual medical assistant from Care VMA can be trained to assist with meticulous time-tracking for E/M and telehealth visits. Our audit services identify missed opportunities in capturing all billable time for these exempt services, helping to balance and offset the revenue loss from surgical and diagnostic codes.
Ensuring AI-Ready Documentation for Full Reimbursement
You can’t bill for the new AI diagnostic codes if your documentation doesn’t support them. Care VMA provides physicians and their teams with specialized documentation templates and training modules. Our Virtual Medical Scribes are experts in ensuring that the provider’s note clearly reflects the use of AI-augmented tools, justifying the use of these new, higher-value Category I codes and securing proper reimbursement.
Feeling overwhelmed by these changes? Download our free checklist: ’10 Steps for 2026 Reimbursement Readiness’ to get started.
Why This All Matters: The Long-Term Impact of Coding Compliance
The day-to-day grind of medical coding can make it easy to lose sight of the bigger picture. But getting your coding and reimbursement right has long-term benefits that ripple across your entire practice, going far beyond just clean claims.
- Improved Cash Flow: Clean claims submitted correctly the first time mean faster payments from payers and a significant reduction in your accounts receivable (A/R) days.
- Reduced Administrative Burden: When denials decrease, your team spends less time on frustrating rework, appeals, and phone calls with payers, freeing them up for higher-value tasks. You can learn more about how a virtual medical admin assistant can reduce this burden.
- Better Data for Payer Negotiations: Accurate coding provides clean, reliable data that strengthens your negotiating position with private payers, allowing you to argue for better contract rates based on the true complexity of your patient population.
- Enhanced Patient Care: At the end of the day, an efficient revenue cycle means a more stable practice. This allows your clinical providers to focus their energy on what matters most: delivering excellent patient care.
The Traditional Approach vs A Care VMA Partnership
Managing these annual changes the old way is no longer sustainable for a growing practice. Relying on manual updates and reactive denial management is a recipe for staff burnout and revenue leakage. Here’s a side-by-side look at the difference a strategic partnership with Care VMA makes.
| Task | Manual In-House Management | Strategic Partnership with Care VMA |
|---|---|---|
| Code Updates | Manual data entry from spreadsheets; high risk of human error. | Automated platform updates pushed in real-time; centralized source of truth. |
| Denial Management | Reactive; team works denials after they’ve already impacted cash flow. | Proactive; custom edits and pre-submission scrubs prevent denials from happening. |
| Staff Training | Fragmented and time-consuming; pulls staff away from core duties. | Structured, expert-led training on specific changes like LER and AI documentation. |
| Overall Cost | High hidden costs (staff salaries, lost time, lost revenue from errors). | Transparent, predictable cost with a clear and measurable return on investment (ROI). |
FAQ (Frequently Asked Questions)
What is a “conversion factor” in medical reimbursement?
The conversion factor (CF) is a dollar multiplier set by CMS each year. It is the final step in the payment formula, converting a procedure’s total Relative Value Units (RVUs) into an actual dollar payment amount. For 2026, CMS has controversially established two different CFs depending on a provider’s participation in an Alternative Payment Model (APM). You can find more details on the official CMS website.
How do I know which CPT codes are in the “global surgical package”?
Every surgical CPT code is assigned a global period indicator (0, 10, or 90 days) within the Medicare Physician Fee Schedule database. This indicator defines the number of days of pre- and post-operative care that are bundled into the payment for the original procedure. You can look up any code on the CMS fee schedule lookup tool or use a modern coding software that automatically displays this information.
Does the -2.5% efficiency cut apply to all CPT codes?
No, it does not. According to the 2026 MPFS Final Rule, this reduction specifically targets the work RVUs of services that are not time-based. This primarily includes most surgical procedures and diagnostic tests. Critically, standard time-based E/M visits and many behavioral health services are exempt from this particular cut for 2026.
Your Path to a Financially Secure 2026
The 2026 CPT and CMS changes are undoubtedly challenging, but they also present a unique opportunity to modernize and optimize your practice’s revenue cycle. By shifting from a reactive mindset to a proactive strategy with the right partner, you can transform this annual compliance burden into a lasting financial advantage.
Ready to see exactly how your practice can adapt and thrive? Schedule a no-obligation, 15-minute demo to see our platform and certified team in action.
Don’t let your 2026 revenue become a casualty of these new rules. Claim your free Reimbursement Readiness Audit today. Our expert team will analyze your top 10 most-billed claims and identify hidden revenue risks from the 2026 updates—at absolutely no cost to you.
