
ragmented patient handoffs are a quiet but persistent crisis in modern healthcare, leading to medical errors, costly hospital readmissions, and an immense burden on clinical teams. What most people don’t realize is that these failures aren’t just a threat to patient safety; they represent a multi-billion dollar problem, directly impacting your facility’s financial health through significant CMS penalties and reputational damage. The solution lies in moving beyond patchwork fixes and implementing a proven, systematic framework for Transitions of Care (TOC) that transforms this critical vulnerability into a process that is safe, efficient, and operationally sound.
Transitions of Care (TOC) is the comprehensive process of moving a patient between different healthcare settings, practitioners, or levels of care as their condition evolves. An effective TOC program is essential for preventing medical errors, reducing preventable hospital readmissions, and ensuring the continuity of care through key components like medication reconciliation, patient education, and standardized communication between providers. This guide is built upon the latest 2026 standards from the Centers for Medicare & Medicaid Services (CMS), The Joint Commission (TJC), and evidence-based models from the Agency for Healthcare Research and Quality (AHRQ).
Why Poor Transitions of Care is a Multi-Billion Dollar Problem?

It’s a figure that should stop every hospital administrator in their tracks: up to 80% of serious medical errors involve miscommunication during the handoff between providers. This isn’t just a patient safety issue; it’s a profound financial liability. Preventable hospital readmissions cost the US healthcare system billions of dollars annually, a cost that is increasingly being passed directly back to facilities.
The financial impact is twofold:
- Direct Penalties: The CMS Hospital Readmissions Reduction Program (HRRP) imposes direct financial penalties on hospitals with higher-than-expected readmission rates for specific conditions. In many cases, a single preventable readmission can wipe out the entire margin from the initial hospitalization.
- Operational Strain: Failed transitions create a cascade of inefficient work. Your team is forced to spend valuable time chasing down records, correcting medication errors, and dealing with frustrated patients and families, all of which contributes to clinical burnout and detracts from providing high-quality care.
The Four Pillars of an Effective TOC Program
Before diving into complex clinical models, it’s crucial to understand the foundational principles that support every patient’s journey home. The widely-adopted Coleman Care Transitions Intervention® provides a simple yet powerful framework built on four pillars. From a provider’s perspective, achieving success in each of these areas builds a bridge to safer post-discharge outcomes.
- Pillar 1: Medication Management: This is the most critical pillar. The goal is to ensure patients not only have their new prescriptions but also clearly understand what to take, what to stop taking, and the purpose of each medication. A thorough medication reconciliation process is non-negotiable here.
- Pillar 2: Patient-Centered Health Record: Patients should leave with a clear, understandable summary of their care, often called an After Hospital Care Plan (AHCP). This empowers them to be active participants in their own health and provides a vital communication tool for their next provider.
- Pillar 3: Follow-Up Appointments: Simply telling a patient to “follow up with your PCP” is not enough. Effective programs ensure appointments are scheduled—and transportation is considered—before the patient is discharged.
- Pillar 4: Knowledge of “Red Flags”: Patients and their caregivers must be educated on how to identify worsening symptoms and know exactly who to call and when. This proactive step can prevent a minor issue from escalating into an emergency department visit or another admission.
Evidence-Based Models: The Clinical Blueprints for Success
Theory is one thing, but proven clinical results are another. High-performing health systems don’t leave transitions to chance; they implement evidence-based models that serve as a blueprint for safe, standardized care. What most people don’t realize is that these models share common components, but each has a unique focus.
Project RED (Re-Engineered Discharge)
Think of Project RED as the ultimate 12-step checklist for a perfect discharge. Developed with funding from the Agency for Healthcare Research and Quality (AHRQ), its cornerstone is the After Hospital Care Plan (AHCP), a patient-friendly document detailing their diagnosis, medication plan, and follow-up appointments. Crucially, the model includes a structured post-discharge phone call to reinforce the plan and address patient questions. Studies have shown Project RED can reduce hospital readmissions by as much as 30%.
Project BOOST (Better Outcomes by Optimizing Safe Transitions)
The focus of Project BOOST is early risk identification. It provides tools to help clinical teams identify high-risk patients at the time of admission, allowing for targeted interventions throughout their stay. The framework uses tools like the 8P’s Risk Assessment to pinpoint vulnerabilities (e.g., polypharmacy, poor health literacy, lack of social support) that could jeopardize a safe discharge.
The Transitional Care Model (TCM)
This model provides intensive, nurse-led support for high-risk, chronically ill older adults. An Advanced Practice Nurse (APN) or “transition coach” follows the patient from the hospital to their home, providing hands-on coordination and management for a period of 1 to 3 months. It is one of the most resource-intensive models but has demonstrated significant success in complex patient populations.
The Operational Blindspot: From Theory to Reality with Care VMA 🔥
Here’s the thing: knowing the blueprint for a perfect discharge and actually executing it on a busy Friday afternoon are two very different challenges. The evidence-based models are the “what,” but the real-world struggle lies in the “how.” This is the operational blindspot, where EHR information silos, staffing shortages, and fragmented communication cause even the best-laid plans to fail. This is where Care VMA becomes the “operational engine” that brings the blueprints to life.
We don’t just talk about the models; we execute them.
Integrasi Care VMA:
- We Bridge Information Silos: Our Virtual Medical Assistants (VMAs) act as a digital hub, ensuring the discharge summary and final medication reconciliation list are transmitted to the PCP instantly, regardless of differing EHR systems. We eliminate the “fax and pray” method.
- We Own the Coordination Burden: Instead of placing another task on your nurses, our VMA team proactively makes the post-discharge phone calls within 2 business days. We confirm follow-up appointments, use the Teach-Back Method to verify patient understanding, and ensure they have access to their medications, freeing up your staff to focus on in-house patients.
- We Automate Accountability: Our platform provides a clear, real-time dashboard tracking every step of the transition. This completely eliminates the “gray zone” of accountability, where the hospital team thinks the outpatient team is handling a task, and vice-versa.
A real-world example: A hospitalist discharges a heart failure patient on a Friday. Traditionally, the PCP might not see the discharge summary until Monday or Tuesday. With Care VMA, the PCP receives a real-time notification with the full clinical summary, and our VMA has already confirmed the 7-day follow-up appointment before the patient even arrives home. Many providers we work with find this level of proactive coordination to be a game-changer for improving patient outcomes.
Unlocking Revenue: Mastering CMS Transitional Care Management (TCM) Billing for 2026
Beyond superior patient safety, a well-executed TOC program isn’t a cost center—it’s a significant revenue opportunity hiding in plain sight. The Centers for Medicare & Medicaid Services (CMS) directly reimburses providers for the work involved in managing patients for the first 30 days post-discharge through Transitional Care Management (TCM) codes.
However, the documentation requirements are strict. To bill CPT codes 99495 and 99496, you must prove three components were completed:
- Interactive Contact: Communication (phone, email, or video) with the patient or caregiver within 2 business days of discharge.
- Non-Face-to-Face Services: Performing tasks like care coordination, medication reconciliation, and patient education during the 30-day period.
- Face-to-Face Visit: A required in-person visit within 7 days of discharge (for CPT 99496, high complexity) or 14 days (for CPT 99495, moderate complexity).
Care VMA’s services are designed to automatically perform and document these requirements, ensuring your practice can capture this revenue without adding to your administrative workload. We handle the calls, the coordination, and the scheduling, providing you with the documentation needed for compliant billing.
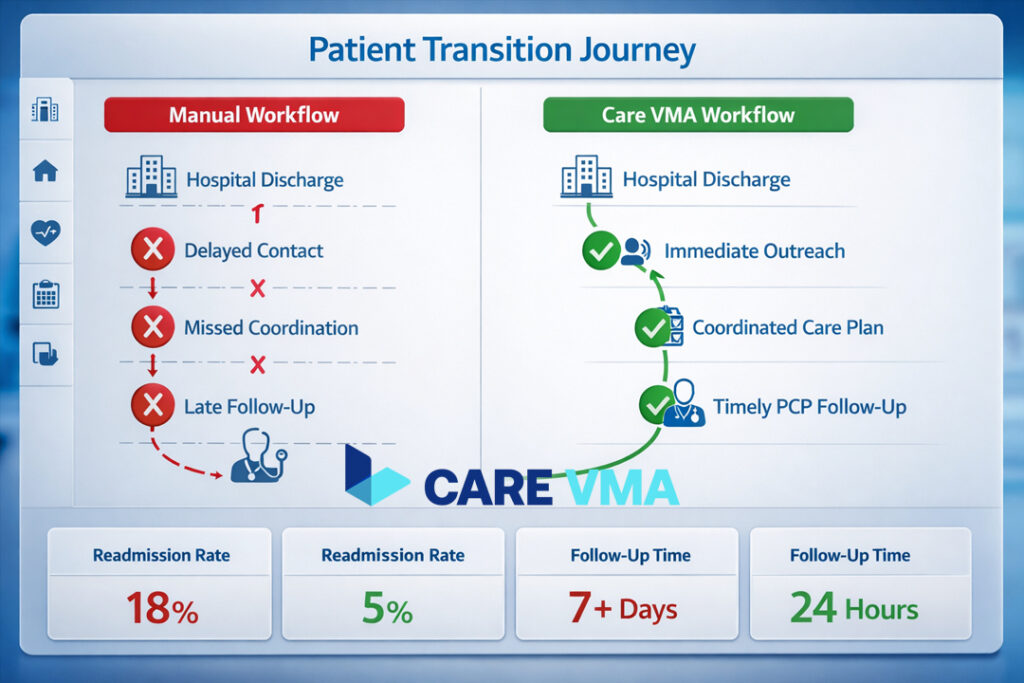
Traditional TOC vs Tech-Enabled TOC with Care VMA
The difference between a TOC process managed by manual effort versus one powered by modern coordination is stark. Here’s a simple breakdown:
| Metric | Traditional Method | With Care VMA |
|---|---|---|
| Communication | Manual, relies on fax & phone tags | Automated, real-time notifications |
| Appointment Coordination | Patient’s responsibility, often missed | Proactively scheduled & confirmed |
| Medication Reconciliation | Prone to human error and delays | Validated & reinforced with education |
| Accountability | Fragmented, “no-man’s land” | Centralized, tracked on a dashboard |
| TCM Billing Opportunity | Often missed due to documentation gaps | Optimized and fully documented |
To further strengthen your practice’s workflows, explore our detailed guides on Medication Reconciliation Best Practices and the 5 Core Strategies to Reduce Hospital Readmissions.
Learn more about how our dedicated teams can help by exploring our Transitional Care Management Services.
Frequently Asked Questions
What are the 4 main pillars in transitions of care?
The four primary pillars are: ensuring safe and effective medication management, providing the patient with a personalized health record or care plan, scheduling and confirming follow-up appointments, and educating the patient on warning signs (“red flags”) that require immediate action.
Who is responsible for the transitions of care process?
TOC is a team responsibility involving doctors, nurses, pharmacists, and case managers. However, effective programs rely on a central coordinator—such as a dedicated case manager or a service like Care VMA—to ensure there are no communication gaps between the discharging hospital and the outpatient providers.
What is the difference between TCM and TOC?
Transitions of Care (TOC) is the broad clinical concept covering the entire process of a patient’s movement between care settings. Transitional Care Management (TCM) refers to a specific set of services, billable to Medicare under CPT codes 99495 & 99496, that cover the management of a patient for the first 30 days after they are discharged from a hospital or skilled nursing facility.
Conclusion
Successfully managing Transitions of Care is no longer about simply knowing the clinical models; it’s about having a reliable operational system to execute them flawlessly every single time. Closing the persistent gaps in communication and accountability is the absolute key to reducing readmissions, ensuring patient safety, and protecting your practice’s financial stability.
Stop letting disconnected manual processes jeopardize your patients and your revenue. It’s time to shift to a structured, automated, and accountable approach.
Ready to turn TOC guidelines into an operational reality? Schedule a 15-Minute Demo to see exactly how the Care VMA Health platform can cut your readmission rates and simplify your team’s workflow.
