
Disclaimer: This article is for informational purposes only and does not constitute professional advice for healthcare administration. Please consult with a qualified expert for guidance specific to your facility’s needs.
A single inaccuracy in a medical document can create significant risks for patient safety and legal compliance. For healthcare managers and clinicians, the pressure to manage thousands of patient records with perfect accuracy while maintaining operational efficiency is immense. This administrative burden contributes to clinician burnout and opens the door to costly errors. The solution lies in a modern documentation and transcription process that blends the speed of technology with the irreplaceable precision of human expertise.
Medical documentation is the systematic recording of a patient’s health information. Medical transcription, a critical component of this process, converts physicians’ oral reports into accurate written text for digital archives and Electronic Health Records (EHRs). This ensures every detail is captured, creating a reliable foundation for patient care.
Dissecting Medical Documentation & Transcription
Think of reliable medical records as a well-built house. Medical documentation is the architectural blueprint, outlining every essential structure. Medical transcription is the process of ensuring every single brick is laid perfectly, creating a solid, dependable structure.
What Is Medical Documentation?
Medical documentation is the comprehensive and chronological record of a patient’s medical history, diagnoses, treatments, and care plans. It includes everything from initial consultation notes to lab results and surgical reports. This documentation serves as the single source of truth for a patient’s health journey.
What Is Medical Transcription?
Medical transcription is the specific task of converting dictated audio notes from healthcare providers into written, formatted documents. This process transforms a physician’s spoken observations into structured data that can be easily integrated into an EHR system, shared among providers, and used for billing and legal purposes.
Why Are They Crucial for Patient Safety and Compliance?
- Ensuring Continuity of Care: Accurate records allow different providers, from primary care physicians to specialists, to have a clear and consistent understanding of the patient’s history, preventing redundant tests and medication errors.
- Legal Basis and Malpractice Protection: Detailed and precise documentation serves as a legal record of the care provided. It protects both the patient and the healthcare facility in the event of legal disputes or audits.
- Billing and Insurance Claim Efficiency: Correctly documented and transcribed records are essential for accurate medical coding, which in turn ensures timely and appropriate reimbursement from insurance payers.
The Evolved Role of the Medical Transcriptionist (Medical Language Specialist)
The role of a medical transcriptionist has evolved far beyond that of a simple typist. In the modern healthcare ecosystem, they are expert data validators and editors, often referred to as Medical Language Specialists. They are the final human checkpoint ensuring the integrity of a patient’s record before it enters the EHR.
Key Responsibilities of a Professional Medical Transcriptionist
- Listening to and Interpreting Medical Dictations: They possess a deep understanding of medical terminology and context to accurately interpret physician dictations.
- Editing Automated (AI) Transcription Outputs: A key task is to review AI-generated drafts, correcting errors in terminology, grammar, and context that automated systems often miss. This editorial function is similar to what a medical scribe does during live encounters, but is applied post-dictation.
- Ensuring Accuracy in Terminology, Grammar, and Formatting: They ensure every document adheres to specific formatting standards required by healthcare facilities and EHR systems.
- Maintaining Confidentiality Under HIPAA Rules: They are rigorously trained in handling Protected Health Information (PHI) in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
Technological Transformation in Medical Transcription: From Speech Recognition to AI
The technology powering medical transcription has undergone a significant transformation, moving from basic tools to intelligent systems that dramatically improve efficiency.
- Speech Recognition Software: The Early Generation Initial speech recognition software was a simple tool that converted spoken words into text. However, it lacked contextual understanding and struggled with accents, various medical terminologies, and background noise, requiring extensive manual editing.
The Smarter Role of Artificial Intelligence (AI)
Modern AI-driven transcription platforms are far more advanced. These systems use machine learning to adapt to a specific doctor’s speech patterns, accent, and vocabulary. They can understand medical context, suggest correct terminology, and learn from corrections made by human editors, becoming more accurate over time.
Cloud-Based Services for Flexible Accessibility
Cloud-based platforms have made transcription services more accessible and scalable. Physicians can dictate from any location using a smartphone or phone line, and the files are securely transmitted to the transcription team. This flexibility allows for faster turnaround times and seamless workflow integration, regardless of physical location.
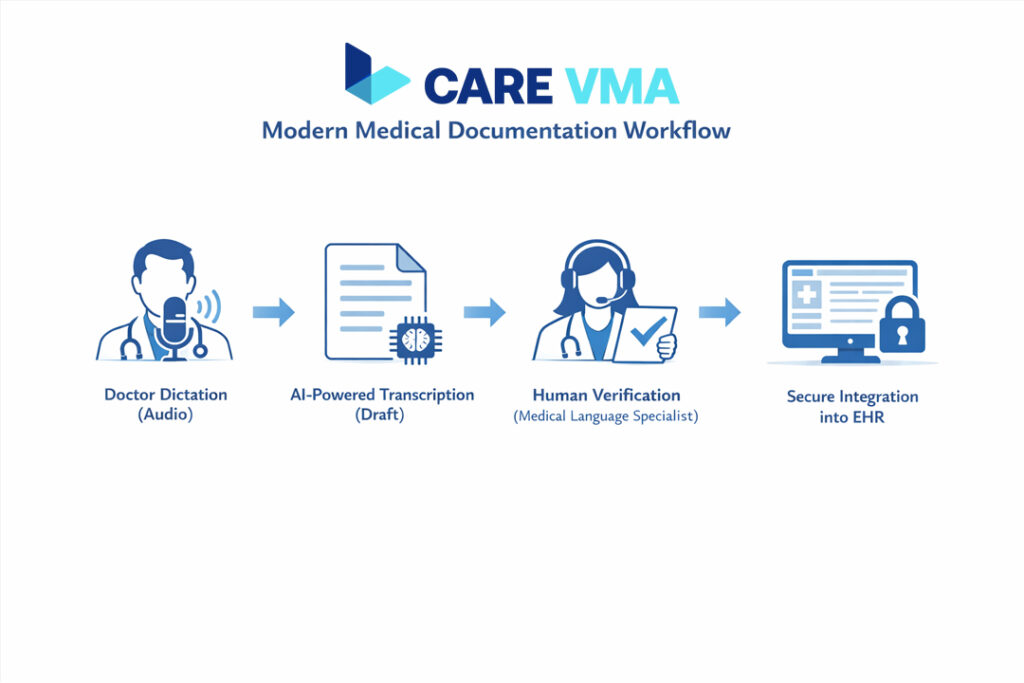
The Synergy of AI and Human Validation: Care VMA’s Fail-Safe Approach
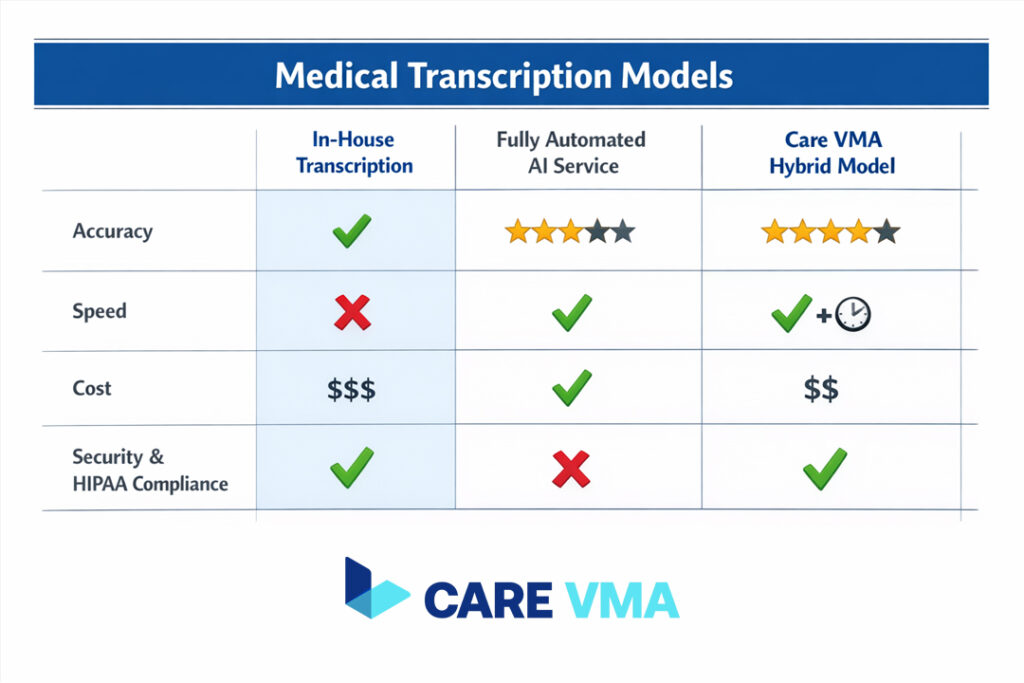
Relying 100% on AI for medical transcription is a high-risk strategy. While fast, automated systems are prone to contextual errors that can have serious consequences. Care VMA’s hybrid model, which combines AI with expert human verification, provides a fail-safe solution that guarantees both speed and unparalleled accuracy.
- The Limitations of AI: Why Contextual Errors Still Occur AI can misinterpret homophones (e.g., “accept” vs. “except”), struggle with thick accents or non-standard dictation styles, and fail to grasp nuanced medical context. An AI might not flag a dosage that seems unusual or a diagnosis that contradicts a patient’s history, as it lacks true clinical judgment.
The Irreplaceable Role of Human Verification
A Medical Language Specialist provides the critical final review. They ensure over 99% accuracy by catching subtle errors, interpreting ambiguous phrases, and guaranteeing that the final document is formatted correctly for seamless EHR and EMR management. This human layer turns a good draft into a legally and clinically sound medical record.
- Mini Case Study: How Validation Prevents a Critical Error A physician dictates “patient has mild hypertension,” but due to a slight mumble, the AI transcribes it as “patient has mild hypotension.” An automated system might let this pass. A human verifier, however, would notice this contradicts the prescribed medication in the patient’s history and flag it for clarification, preventing a potentially dangerous diagnostic error.
Compliance and Security: Protecting Patient Data to HIPAA Standards
In healthcare, data security is not optional. Choosing a transcription service requires strict scrutiny of its security protocols and HIPAA compliance. Care VMA prioritizes data protection as a core component of its service.
Core HIPAA Principles in Medical Documentation HIPAA mandates strict rules for protecting the privacy and security of Protected Health Information (PHI). This includes controlling who can access patient data, how it is stored, and how it is transmitted. Any partner handling PHI must demonstrate robust compliance measures.
Essential Security Protocols for Service Providers
- End-to-End Data Encryption: All audio files and transcribed documents must be encrypted both in transit and at rest, making them unreadable to unauthorized parties.
- Role-Based Access Controls: Only authorized personnel with a legitimate need should be able to access specific patient data. A robust system ensures that access is limited and tracked.
- Audit Trails for Activity Tracking: Every action taken on a document—from viewing to editing—must be logged. This creates an audit trail that is crucial for security and accountability. Our commitment to HIPAA compliance and data security ensures your practice and patients are always protected.
FAQ (Frequently Asked Questions About Medical Documentation & Transcription)
How long does the medical transcription process take?
Standard turnaround time is typically 24 hours. However, STAT (priority) services can complete reports within a few hours, depending on the urgency and complexity of the dictation.
Can transcription services integrate with any EHR system?
Yes, modern providers like Care VMA use standardized formats like HL7 and custom APIs to ensure that transcribed data can be imported seamlessly into nearly all leading EHR systems, preserving data structure and integrity.
How do you ensure accuracy if a doctor has a strong accent?
This is where the hybrid model excels. The AI system generates an initial draft. A trained Medical Language Specialist then listens to the original audio to verify every word, paying special attention to critical terminology and nuances that an automated system might miss due to the accent. This ensures the highest level of accuracy for any dictator.
Conclusion & Next Steps
Accurate medical documentation is not just an administrative task; it is a fundamental pillar of safe, effective, and efficient healthcare delivery. In 2026 and beyond, embracing a modern solution that combines the power of AI with the critical judgment of human experts is the smartest investment a healthcare facility can make. This approach mitigates risk, reduces administrative load on clinicians, and builds a foundation of trustworthy patient data.
Don’t let documentation risks compromise your quality of care. The support of a Virtual Medical Scribe can transform your documentation process, ensuring accuracy and freeing up your team to focus on what matters most—your patients. Schedule a free consultation with Care VMA’s team to analyze your documentation workflow today.
