
![Collaborative Care Model (CoCM): Improve Outcomes & ROI [Guide]](https://carevmahealth.com/wp-content/uploads/2026/03/Collaborative-Care-Model-CoCM-1024x683.jpg)
Running a primary care practice in 2026 feels like an impossible balancing act. Your clinic is overwhelmed with patients presenting with complex mental health needs, from anxiety and depression to substance use concerns. The traditional “refer out” model is clearly broken—it leads to provider burnout, patients getting lost to follow-up, and a frustrating sense of providing incomplete care. This inefficient system doesn’t just hurt your patients; it agitates your entire workflow, affects your quality metrics, and leaves significant revenue on the table from unbilled services.
Now, imagine a system where treating depression is as routine and integrated as managing diabetes. A system where your providers feel supported by a dedicated mental health team, not burdened by it, allowing them to improve both patient outcomes and your practice’s bottom line. This isn’t a future-state dream; it’s the Collaborative Care Model (CoCM).
The Collaborative Care Model (CoCM) is a clinically-proven, team-based approach for integrating mental health services directly into primary care settings. It utilizes a structured, data-driven framework to treat common mental health conditions, significantly improving patient outcomes and practice revenue. This isn’t just another theory. CoCM is the gold-standard model for integrated behavioral health, developed by the University of Washington’s AIMS Center and backed by the American Psychiatric Association (APA) and more than 90 randomized controlled trials.
What is the Collaborative Care Model (And What It’s Not)?
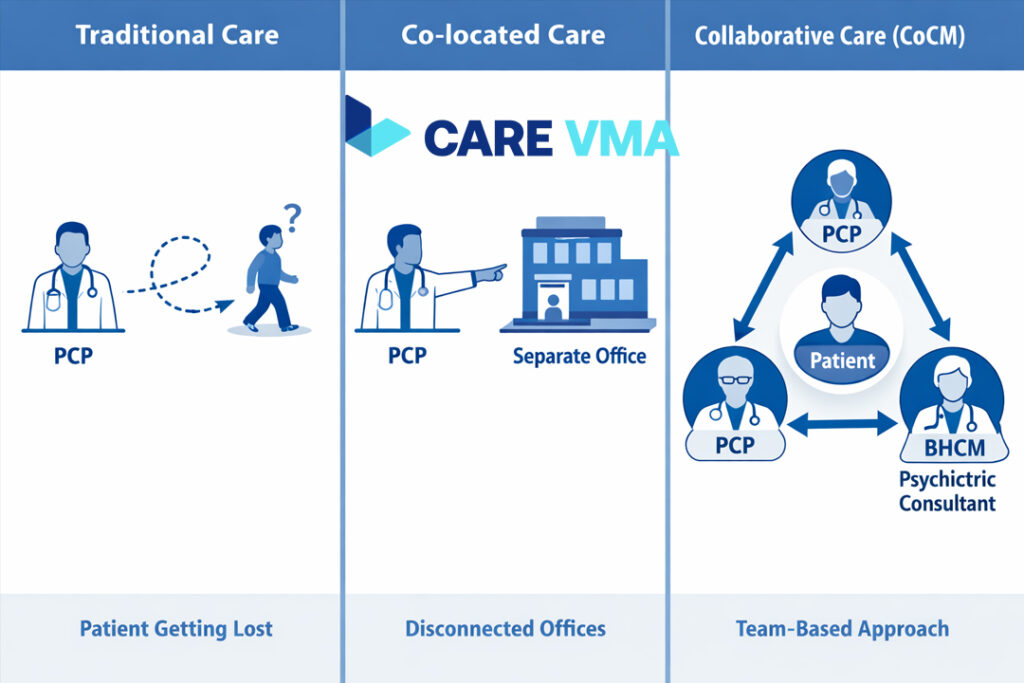
You might have heard the term ‘integrated care’ before, but the Collaborative Care Model is something very specific—and far more effective than simply having a therapist down the hall. At its core, CoCM is about treating mental and behavioral health with the same rigor and structure as any other chronic disease.
What most people don’t realize is that CoCM is defined by five core principles that work together:
- Patient-Centered Team Care: The patient, the Primary Care Provider (PCP), and a Behavioral Health Care Manager (BHCM) work as a cohesive unit, often supported by a psychiatric consultant. The care plan is shared, and the patient is an active participant.
- Population-Based Care: Instead of just managing one-off visits, the team uses a patient registry to track an entire caseload of patients. This ensures no one “falls through the cracks” and allows for proactive outreach.
- Measurement-Based Treatment to Target: Progress isn’t a guessing game. The team uses validated screening tools, like the PHQ-9 for depression or GAD-7 for anxiety, to measure symptoms. Treatment is actively adjusted until the patient reaches their specific clinical goals.
- Evidence-Based Care: CoCM relies on treatments that are proven to work. This typically includes brief psychotherapies like Problem-Solving Treatment or Behavioral Activation and evidence-based medication protocols.
- Accountable Care: The entire team is accountable for the clinical outcomes of their patient population, not just for the volume of services they provide.
A crucial distinction to make is that CoCM is not a “co-located model.” Co-location is when a therapist rents space in your building but works independently. In true Collaborative Care, the providers are a single, integrated team using a shared health record, a unified care plan, and systematic psychiatric oversight to manage patient care together.
The Core Team: Who Does What in Collaborative Care
CoCM isn’t about adding more work to your plate; it’s about adding the right experts to your team to lighten the load and improve effectiveness. This model redesigns the care team into a highly efficient triad.
Primary Care Provider (PCP)
The PCP remains the leader of the patient’s care team. In the CoCM framework, however, their role is enhanced, not burdened. They continue to manage the patient’s overall health and prescribe medications, but they are now supported by a behavioral health specialist who handles the day-to-day management, follow-up, and brief therapy.
Behavioral Health Care Manager (BHCM)
Here’s the thing: the BHCM is the engine of the Collaborative Care team. This team member, often a clinical social worker, nurse, or psychologist, is based in the primary care clinic and is responsible for:
- Maintaining the patient registry and tracking progress.
- Providing evidence-based brief counseling (e.g., behavioral activation, problem-solving therapy).
- Acting as the primary point of contact for the patient between PCP visits.
- Presenting cases to the psychiatric consultant for expert guidance.
Psychiatric Consultant
The psychiatric consultant is the expert guide who provides invaluable support without needing to see patients directly. This is a game-changer for access. They meet with the BHCM weekly (often for just a few hours) to review the patient caseload, providing recommendations for patients who are not improving as expected. This “caseload consultation” model allows one psychiatrist to support the care of hundreds of patients, a level of efficiency impossible in traditional care.
Is CoCM Right for Your Practice? The Business Case & ROI
Beyond delivering superior patient care, does CoCM actually make financial sense for a busy practice? The data is exceptionally compelling. This isn’t just an investment in quality; it’s a direct path to a healthier bottom line and improved provider wellness.
The financial benefits come from two main areas: operational efficiency and new revenue streams. By treating mental health effectively within primary care, you reduce the overall cost of care, prevent costly emergency room visits, and improve management of chronic physical conditions like diabetes and heart disease, which are often exacerbated by untreated depression or anxiety.
The evidence speaks for itself. Multiple studies, including the foundational IMPACT study published in JAMA, have demonstrated the model’s power:
- Patients in CoCM are twice as likely to experience a 50% or greater reduction in depression symptoms.
- The average return on investment (ROI) is $6.50 for every $1 spent on the program, according to an analysis by the University of Washington.
Furthermore, specific billing codes have been established to ensure practices are reimbursed for this high-value work. The main Medicare CPT codes for CoCM (CPT 99492, 99493, and 99494) reimburse for the time spent by the care team managing the patient’s care each month, including non-face-to-face activities like case reviews and chart updates.
Your Step-by-Step CoCM Implementation Roadmap
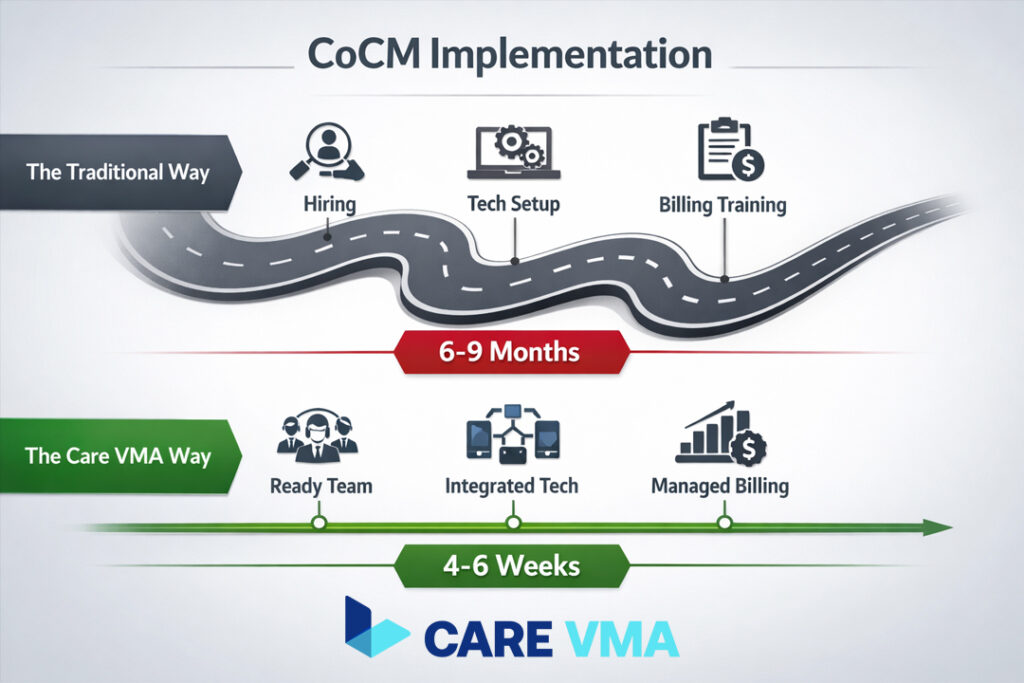
This is where theory meets reality. Implementing CoCM has its hurdles, but it doesn’t have to be a nine-month headache. While the framework is proven, the operational lift—from staffing to technology to billing—is where most practices get stuck. Below is a practical roadmap, highlighting common challenges and showing how a dedicated partner can transform the process.
Phase 1: Preparation & Buy-In
The first step involves getting leadership commitment and assembling your team.
- Common Challenge: Finding, hiring, and training a qualified Behavioral Health Care Manager (BHCM) can take months and is often the biggest barrier. Sourcing a part-time psychiatric consultant can be equally difficult.
- The Care VMA Solution: Forget the recruitment headache. Care VMA provides pre-trained, expert Virtual Patient Care Coordinators who function as your BHCM from day one. We also handle sourcing the psychiatric consultant, giving you an entire clinical team, ready to go.
Phase 2: Workflow & Tech Setup
Next, you need to define your clinical process and get the right tools.
- Common Challenge: Most EHRs lack a built-in patient registry designed for CoCM. Building one from scratch or purchasing standalone software is expensive and creates an IT bottleneck.
- The Care VMA Solution: Our team works within your existing EHR. We provide and manage the compliant patient registry and all documentation, ensuring your team has the data they need without any IT overhead on your part.
Phase 3: Clinical Launch
This is when you begin screening patients and enrolling them in the program.
- Common Challenge: Training your PCPs and front desk staff on new screening and “warm hand-off” protocols adds another layer of work to their already busy schedules, often leading to inconsistent adoption.
- The Care VMA Solution: Our virtual assistants can manage much of this process remotely. They can help with pre-visit screening, scheduling and patient intake, and ensure all necessary information is ready for the PCP, making the clinical launch seamless.
Phase 4: Billing & Sustainability
To ensure the program is sustainable, you must master the billing process.
- Common Challenge: Billing for CoCM is notoriously complex and time-based, requiring meticulous documentation that is easy to get wrong, leading to denied claims and lost revenue.
- The Care VMA Solution: This is our specialty. Our remote medical billing assistants handle all time-tracking, documentation, and claim submission for CoCM codes, ensuring you maximize reimbursement without compliance risks. We turn a complex administrative burden into a reliable new revenue stream.
The Proven Benefits: Better Outcomes for Patients & Providers
So what’s the bottom line for your patients, your providers, and your practice? The benefits of a well-implemented CoCM program are comprehensive and create a virtuous cycle of improvement across your entire organization.
For Your Patients:
- Improved Access to Care: Patients receive mental health treatment in the familiar, non-stigmatizing setting of their primary care office.
- Better Clinical Outcomes: As proven by decades of research, patients achieve remission from depression and anxiety at significantly higher rates.
- Integrated, Whole-Person Care: Mental and physical health are treated in a coordinated fashion, improving overall well-being.
For Your Providers:
- Reduced Burnout: PCPs report higher job satisfaction and less stress when they have a dedicated team to help manage complex behavioral health cases. These solutions for physician burnout are critical for long-term practice stability.
- Expert Support: Having direct access to a psychiatric consultant for guidance on tough cases builds PCP confidence and clinical skills.
- Focus on Top-of-License Work: PCPs can focus on diagnosis and medical treatment plans, knowing the BHCM is handling follow-up and counseling.
For Your Practice:
- Increased Revenue: New, sustainable revenue streams are generated through CoCM billing codes.
- Improved Quality Metrics: Practices see better performance on key HEDIS and quality measures related to depression screening and management.
- Competitive Advantage: Offering gold-standard integrated care makes your practice a more attractive choice for both patients and potential new providers.
Frequently Asked Questions about Collaborative Care
Who can be a Behavioral Health Care Manager (BHCM)?
A BHCM is a clinical professional with specific training in brief, evidence-based therapies. Most commonly, they are Licensed Clinical Social Workers (LCSW), Licensed Professional Counselors (LPC), psychologists, or Registered Nurses (RN) with behavioral health training.
How much time does the Psychiatric Consultant need?
Typically, a psychiatric consultant dedicates about 2-4 hours per week for every 100 patients in the practice’s CoCM caseload. They do not see patients directly but use this time to conduct the weekly caseload review with the BHCM and provide expert recommendations.
What are the main CPT codes for CoCM?
The primary Medicare CPT codes are 99492 (for the first 70 minutes of clinical staff time in the initial month), 99493 (for the first 60 minutes in subsequent months), and 99494 (for each additional 30 minutes). These codes are designed to reimburse for the total time the team spends on the patient’s care each month.
Conclusion
You don’t have to reinvent the wheel to solve your mental health integration problem. The Collaborative Care Model provides a proven, evidence-based roadmap to transform your practice, reduce provider burnout, and deliver the gold-standard of integrated care your patients deserve. The question isn’t whether CoCM works—it’s how to implement it without disrupting your practice and overwhelming your team.
Ready to finally bridge the gap between knowing and doing?
Stop struggling with implementation. Stop losing revenue to complex billing. Stop letting your providers burn out. Care VMA provides the trained virtual staff, compliant technology, and billing expertise to launch your Collaborative Care program in weeks, not months.
